Note: This is a repost from 2019-very relevant for today.
Definition of Terminal:
Terminal condition means an incurable and irreversible condition, for the end stage of which there is no known treatment which will alter its course to death, and in the opinion of the attending physician in that disease category, will result in premature death.
Terminality is defined as having a condition that is irreversible and will result in premature death, someone like Joni Eareckson Tada would fit that description, as well as thousands of other’s with disabilities, in wheelchairs, and chronic diseases, such as those on kidney dialysis. None of them are dying, but are living in a terminal state.
Health Insurance is a very big issue-a big area of misuse and abuse-especially with family members involved. For example:
Loopholes for Health Insurance Plans
In Oregon, people labeled as “terminal”, can be denied coverage for treatment, but have been offered coverage for suicide instead. For instance, the case of Barbara Wagner, who had lung cancer. The Oregon Health Plan refused to pay for a drug that would possibly prolong her life, but offered to pay for her suicide instead.
Elder abuse is often difficult to detect. This is largely due to the unwillingness of victims to report. "Shame, dependence on the abuser, fear of retribution, and isolation from the community are significant obstacles that discourage elders from reporting … "
Definition of Terminal:
Terminal condition means an incurable and irreversible condition, for the end stage of which there is no known treatment which will alter its course to death, and in the opinion of the attending physician in that disease category, will result in premature death.
Terminality is defined as having a condition that is irreversible and will result in premature death, someone like Joni Eareckson Tada would fit that description, as well as thousands of other’s with disabilities, in wheelchairs, and chronic diseases, such as those on kidney dialysis. None of them are dying, but are living in a terminal state.
Health Insurance is a very big issue-a big area of misuse and abuse-especially with family members involved. For example:
Loopholes for Health Insurance Plans
In Oregon, people labeled as “terminal”, can be denied coverage for treatment, but have been offered coverage for suicide instead. For instance, the case of Barbara Wagner, who had lung cancer. The Oregon Health Plan refused to pay for a drug that would possibly prolong her life, but offered to pay for her suicide instead.
Elder abuse is often difficult to detect. This is largely due to the unwillingness of victims to report. "Shame, dependence on the abuser, fear of retribution, and isolation from the community are significant obstacles that discourage elders from reporting … "

What Is My Stand on Physician Assisted Suicide and Euthanasia
Euthanasia involves the intentional killing of a patient by the direct intervention of a physician or another party, ostensibly for the good of the patient or others. The most common form of euthanasia is lethal injection. Euthanasia can be voluntary (at the patient's request), non-voluntary (without the knowledge or consent of the patient) or involuntary (against his or her wishes).
The bottom line of this is, it is killing-going totally against the sixth commandment in the bible- Thou shall not kill. Ex 20:13
Legalization of assisted suicide is a recipe for elder abuse. It devalues people with disabilities. Its promise of individual choice is an illusion.
Policy debates around this question generally fall into two categories: physician-assisted suicide and euthanasia. These terms are often used interchangeably; however, the distinctions are significant. The act of physician-assisted suicide involves a medical doctor who provides a patient the means to kill him or herself, usually by an overdose of prescription medication.
Physician-assisted suicide and euthanasia violate the sanctity of human life.
People living with terminal illness deserve more than the offer of a physician to facilitate their death. They merit true compassion. Accessing expert palliative (hospice) care and comfort care — treating the symptoms and making the patient as comfortable as possible during the natural dying process. Palliative (hospice) care differs from acute care in that it becomes appropriate when aggressive therapies are no longer beneficial to the patient and there is no longer an attempt to cure the disease.
Barriers need to be removed that prevent patients from receiving available treatments for pain and other symptoms — not alleviate the safeguards that protect patients from psychological or financial coercion to choose an untimely death. The goal should not be to legalize physician-assisted suicide but rather to adequately provide available means of care so that patients and their families do not feel the need to consider an early death.
Euthanasia involves the intentional killing of a patient by the direct intervention of a physician or another party, ostensibly for the good of the patient or others. The most common form of euthanasia is lethal injection. Euthanasia can be voluntary (at the patient's request), non-voluntary (without the knowledge or consent of the patient) or involuntary (against his or her wishes).
The bottom line of this is, it is killing-going totally against the sixth commandment in the bible- Thou shall not kill. Ex 20:13
Legalization of assisted suicide is a recipe for elder abuse. It devalues people with disabilities. Its promise of individual choice is an illusion.
Policy debates around this question generally fall into two categories: physician-assisted suicide and euthanasia. These terms are often used interchangeably; however, the distinctions are significant. The act of physician-assisted suicide involves a medical doctor who provides a patient the means to kill him or herself, usually by an overdose of prescription medication.
Physician-assisted suicide and euthanasia violate the sanctity of human life.
People living with terminal illness deserve more than the offer of a physician to facilitate their death. They merit true compassion. Accessing expert palliative (hospice) care and comfort care — treating the symptoms and making the patient as comfortable as possible during the natural dying process. Palliative (hospice) care differs from acute care in that it becomes appropriate when aggressive therapies are no longer beneficial to the patient and there is no longer an attempt to cure the disease.
Barriers need to be removed that prevent patients from receiving available treatments for pain and other symptoms — not alleviate the safeguards that protect patients from psychological or financial coercion to choose an untimely death. The goal should not be to legalize physician-assisted suicide but rather to adequately provide available means of care so that patients and their families do not feel the need to consider an early death.
What Results in the Legalization of Assisted Suicide
Assisted suicide is a half-way house, a stop on the way to other forms of direct euthanasia, for example, for incompetent patients by advance directive or suicide in the elderly. So, too, is voluntary euthanasia a half-way house to involuntary and non-voluntary euthanasia. If terminating life is a benefit, the reasoning goes, why should euthanasia be limited only to those who can give consent? Why need we ask for consent?"
It must be recognized that assisted suicide and euthanasia will be practiced through the prism of social inequality and prejudice that characterizes the delivery of services in all segments of society, including health care. Those who will be most vulnerable to abuse, error, or indifference are the poor, minorities, and those who are least educated and least empowered. This risk does not reflect a judgment that physicians are more prejudiced or influenced by race and class than the rest of society - only that they are not exempt from the prejudices manifest in other areas of our collective life.
While our society aspires to eradicate discrimination and the most punishing effects of poverty in employment practices, housing, education, and law enforcement, we consistently fall short of our goals. The costs of this failure with assisted suicide and euthanasia would be extreme. Nor is there any reason to believe that the practices, whatever safeguards are erected, will be unaffected by the broader social and medical context in which they will be operating. This assumption is naive and unsupportable."
Above and beyond all of this; the question is, what does God think of this?
To the unbeliever, once you die that's it, no memory of this life, and you simply cease to exist. The truth is, we exist forever, either in heaven with God, or hell. The choices we make in this life, and what we do with Jesus Christ will determine where we will spend eternity. Scriptures teaches:
Heb 9:27 And as it is appointed unto men once to die, but after this the judgment:
When we stand before God, we will give an account for every decision we've made-whether it be good or evil. God's commands regarding life are clear:
Exo 20:13 Thou shalt not kill.
Deu 5:17 Thou shalt not kill.
- Social acceptance of physician-assisted suicide sends the message that some lives, especially those of elderly, disabled and dependent citizens, have less value, and are not worth living.
- Better medical alternatives exist to physician-assisted suicide. However, they are not brought to the light as much as they should, family members need to be more engaged, and aggressive in becoming informed to the resources available. Today's pain management techniques can provide relief for up to 95 percent of patients, thus offering true death with dignity.
- Physician-assisted suicide often ignores anxiety, depression, and family problems, which is a legitimate cry for help.
- Physician-assisted suicide gives too much power to doctors, threatening patient autonomy by allowing physicians to decide whether a patient lives or dies. This is occurring now in the Netherlands, Europe.
- The practice of physician-assisted suicide threatens to destroy the delicate trust relationship between doctor and patient – a relationship based on the patient's belief that his or her physician will pursue the goal of protecting life.
- Physician-assisted suicide opens the door to euthanasia. Then, when this boundary is overstepped, where is this going to lead? Where will this mindset go next? Who else will be termed “better off dead?”
Assisted suicide is a half-way house, a stop on the way to other forms of direct euthanasia, for example, for incompetent patients by advance directive or suicide in the elderly. So, too, is voluntary euthanasia a half-way house to involuntary and non-voluntary euthanasia. If terminating life is a benefit, the reasoning goes, why should euthanasia be limited only to those who can give consent? Why need we ask for consent?"
It must be recognized that assisted suicide and euthanasia will be practiced through the prism of social inequality and prejudice that characterizes the delivery of services in all segments of society, including health care. Those who will be most vulnerable to abuse, error, or indifference are the poor, minorities, and those who are least educated and least empowered. This risk does not reflect a judgment that physicians are more prejudiced or influenced by race and class than the rest of society - only that they are not exempt from the prejudices manifest in other areas of our collective life.
While our society aspires to eradicate discrimination and the most punishing effects of poverty in employment practices, housing, education, and law enforcement, we consistently fall short of our goals. The costs of this failure with assisted suicide and euthanasia would be extreme. Nor is there any reason to believe that the practices, whatever safeguards are erected, will be unaffected by the broader social and medical context in which they will be operating. This assumption is naive and unsupportable."
Above and beyond all of this; the question is, what does God think of this?
To the unbeliever, once you die that's it, no memory of this life, and you simply cease to exist. The truth is, we exist forever, either in heaven with God, or hell. The choices we make in this life, and what we do with Jesus Christ will determine where we will spend eternity. Scriptures teaches:
Heb 9:27 And as it is appointed unto men once to die, but after this the judgment:
When we stand before God, we will give an account for every decision we've made-whether it be good or evil. God's commands regarding life are clear:
Exo 20:13 Thou shalt not kill.
Deu 5:17 Thou shalt not kill.
In the years I took care of elders, many of them went through the valley of suffering, losing strength and their health, and faced death. But there were medications, procedures, and treatments available that allowed them to go through their end days to a great degree without pain. I took care of many in this situation, and my mother until her death, and many years with my husband as he dealt with heart disease, til his death. No one enjoys the pain and suffering involved in these realities. But, the value of human life must be taken into account.
When you know God has created each individual, and the value he puts on every person, and know that the commandment to no kill is still His word to us today-it brings a perspective to the extent we are expected to go to give that person as much care and dignity possible.
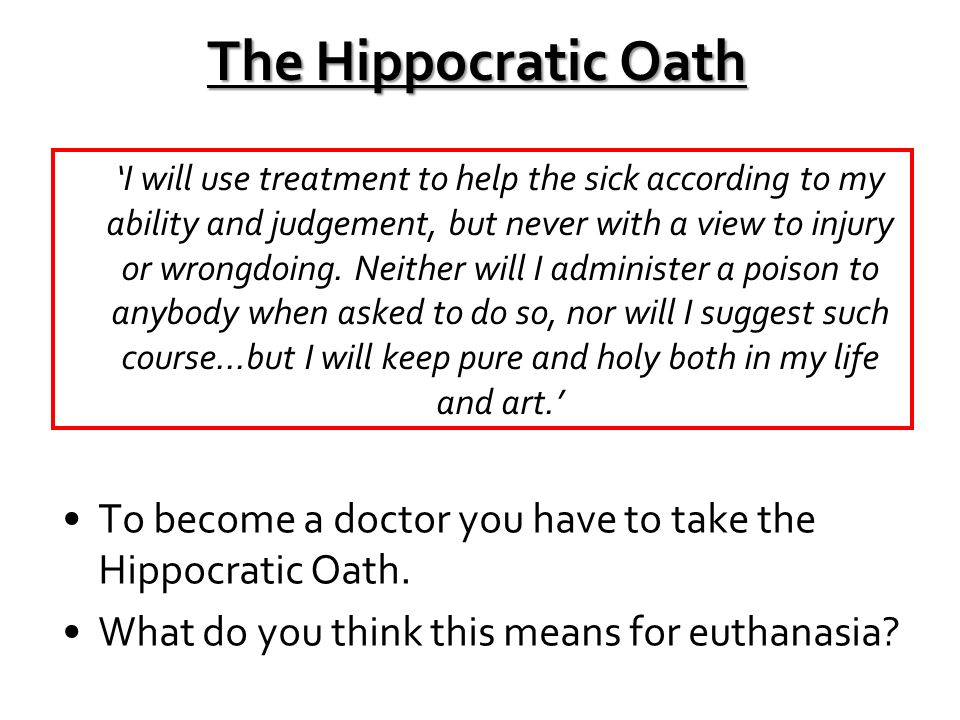
The Hippocratic Oath needs to be reinstated in the medical profession, and not altered to allow this evil practice.
My concern is also for the doctor's and nurses who give in to this practice of legalized murder, and play God every time they end a life by injecting the poison to kill. Over time, if they ever had a soul with a conscience, they must come to the place of having trouble living with what they do-as the numbers of people they kill adds up. If it doesn't, it can be compared to the Nazi ovens, and concentration camps, and the murder and carnage that took place there at that time. I see no difference really-and foresee us coming to that time of barbarism again with these laws being put into place, not just here but around the world. Think about it.
Lorna Couillard
When you know God has created each individual, and the value he puts on every person, and know that the commandment to no kill is still His word to us today-it brings a perspective to the extent we are expected to go to give that person as much care and dignity possible.
The Hippocratic Oath needs to be reinstated in the medical profession, and not altered to allow this evil practice.
My concern is also for the doctor's and nurses who give in to this practice of legalized murder, and play God every time they end a life by injecting the poison to kill. Over time, if they ever had a soul with a conscience, they must come to the place of having trouble living with what they do-as the numbers of people they kill adds up. If it doesn't, it can be compared to the Nazi ovens, and concentration camps, and the murder and carnage that took place there at that time. I see no difference really-and foresee us coming to that time of barbarism again with these laws being put into place, not just here but around the world. Think about it.
Lorna Couillard